


Global COVID-19 responses: 'Zero COVID-19 Case Policy' vs. 'Coexisting with COVID-19 Policy'











(1) Lockdown policy
On Jan. 23, 2020, Wuhan in Hubei province suspended public transportation, closed airports, train stations and other routes leaving it, and asked people not to go outside the city, beginning the so-called lockdown[9]. On Jan. 24, the next day, the whole province activated the first-level response mechanism for major public health emergencies according to the Response Plan for Public Health Emergencies in Hubei province[10]. The response level specifies the degree of various measures to be taken in the identified infected area, and the first-level response requires to suspend work, classes and traffic to avoid any possible personnel flow and close contact[11].
As the upper-level regulation of the Response Plan for Public Health Emergencies of various provinces, municipalities and autonomous regions, the National Response Plan for Public Health Emergencies was formulated based on the experience of combating SARS, and was announced on June 26, 2006, as one of the nation's responses to public health emergencies[12].
Subsequently, other provinces, municipalities and autonomous regions also activated the first-level response mechanism. As of Jan. 29, after the Tibet Autonomous Region activated it, all regions in the entire country had implemented the first-level response mechanism.
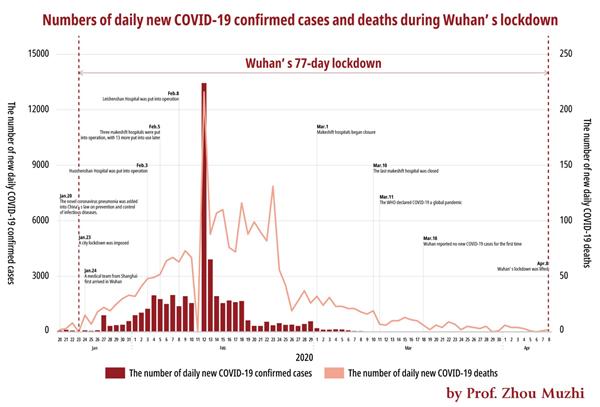
Note 1: There is no data for Jan. 23, the day when the city began the lockdown, as well as data for Feb. 11. The number of confirmed cases surged on Feb. 12, presumably because it was added up by the figures of the previous day.
Source: The official website of the Health Commission of Hubei province.
Chart 2 shows the numbers of new confirmed COVID-19 cases and deaths in Wuhan every day from Jan. 20, days before the lockdown, to Apr. 8, the day when the lockdown was lifted. On Feb. 13, 21 days after the lockdown, Wuhan finally began to see a decline in its daily number of new cases after overcoming various difficulties caused by an unknown virus outbreak, such as the collapse of medical system. On Mar. 18, 56 days after the lockdown, the figure was brought down to zero for the first time. Although a case was confirmed on Mar. 23, the figure remained to be zero for 16 consecutive days until the lockdown was lifted on Apr. 8.
It was undoubtedly a powerful move to lock down the city by cutting off traffic, suspending work, production and classes, and putting in place other measures strictly restricting personnel flow and close contact. Wuhan finally managed to fight back the novel coronavirus after 77 days of lockdown.
China saw the effects of its strict restriction measures throughout the country soon, and its new confirmed cases were quickly brought under control. On Feb. 21, Gansu province took the lead in lowering the response level from the first level to the third and resuming everyday production and life conditionally. Other regions also lowered their response levels from the first to the third since then. On June 13, as Hubei province lowered the level from the first to the third, the response levels across the country were brought down to the third. China has successfully addressed the first wave of COVID-19 thanks to the strict lockdown rules that brought the number of infected cases down to zero.
After that, various parts of China flexibly adjusted their response levels based on local epidemic situations. For example, Beijing raised its response level from the third to the second on June 16 due to a cluster of cases, and strengthened its epidemic prevention and control. As the epidemic was brought under control, Beijing lowered its response level back to the third on July 20.
(2) Quick dispatch of medics
In response to the serious shortage of medical personnel in Wuhan and their drop in number, the Chinese government quickly mobilized a large number of medical staff from all over the country to assist Wuhan. On Jan. 24, 2020, the second day after the lockdown, the Shanghai medical team to assist Wuhan arrived in the city first. It was made up of 136 doctors and nurses from the respiratory departments, infectious disease departments, hospital infection management departments and intensive care medicine departments of 52 hospitals in Shanghai. Eventually, 346 medical teams involving 42,600 medical workers were dispatched to Wuhan and other parts of Hubei province.
The Joint Prevention and Control Mechanism of the State Council introduced at a press conference on Mar. 8 that it usually takes no more than two hours from the time a medical institution receives an order to the time a medical team is set up, and takes no more than 24 hours from the assembly of medical team members to their arrival in Wuhan. The emergency assistance quickly alleviated the pressure on Wuhan in medical terms and effectively saved the city's medical system from collapsing.
It is certain that whether a country can offer its affected area rapid and effective assistance or not is one of the keys to winning over the epidemic, but not all countries are equipped with such capabilities. Judging from the situation in New York and Tokyo, even developed countries with relatively abundant medical resources would find it difficult to mobilize a sufficient number of medical staff to offer assistance in time.
What is even more worrying are those developing countries with a severe shortage of medical resources. Leaving Africa aside, even the neighboring Asian developing countries with large populations, like India and Indonesia, have only 0.8 doctors and 0.3 doctors, and 0.5 beds and one bed in medical facilities, per thousand people, respectively. In such countries with scarce medical resources and insufficient capabilities to offer national assistance, the scramble for medical resources caused by epidemic outbreaks may be extremely severe. Therefore, it is extremely urgent to organize global assistance. The problem is that most developed countries are also suffering from the COVID-19 pandemic and can spare no time to take care of others. At this moment, China's medical assistance to other countries is particularly valuable.
(3) Rapid construction of makeshift hospitals
Wuhan rush-built the Huoshenshan Hospital and the Leishenshan Hospital for severe cases under national support. The two hospitals with high isolation levels are equipped with specialized treatment equipment, and 1,000 beds and 1,600 beds, respectively. The Huoshenshan Hospital opened on Feb. 3, 12 days after the lockdown, and the Leishenshan Hospital was put into use on Feb. 8.
The city also converted stadiums into 16 makeshift hospitals for treating mild cases, and quickly provided 13,000 beds with antibacterial and epidemic prevention levels up to those of first-class hospitals in China. The move channeled mild cases, helping to concentrate high-end medical resources on severe cases, and alleviated the scramble for medical resources.
The experience of Wuhan—building Huoshenshan, Leishenshan and temporary treatment centers to address bed shortage—is worthy of reference and learning for the world.
During the first wave of the COVID-19 pandemic, Japan required some confirmed patients to stay at home for quarantine due to insufficient beds, which was actually an extremely dangerous practice. First, it put the family members of the patients at risk and might lead to infections in clusters within the families. Second, patients could not get effective and professional treatment, and without timely update on health conditions, they might not be able to receive swift referral for treatment when the conditions deteriorated. Fortunately, the practice was largely halted later, and Japan now has also transformed facilities like hotels into isolation wards for patients with mild symptoms, in an effort to channel mild cases and relieve the pressure on hospitals.
A more serious problem in Tokyo is the shortage of ICUs. By 2018, Japan had merely 4.3 ICU beds per 100,000 people, and there was a huge gap compared with the 35 in the US, 30 in Germany, 11.6 in France, 12.5 in Italy, and 9.7 in Spain.
Tokyo, which had the largest number of infected cases in Japan, had only 764 ICU beds, or only 5.5 per 100,000 people, when the first outbreak took place. Through various efforts, Tokyo addressed the serious shortage of ICU beds and survived the first wave. However, as the second wave arrives in autumn and winter, there will be a shortage again. A proper solution to it is a key to avoiding a potential collapse of its medical system amid an outbreak.
The countries have adopted a variety of measures to address bed shortage during the outbreaks, with the US even sending naval hospital ships to assist[13]and South Korea taking the emergency importation of a "hospital" as a new option. Faced with a desperate shortage of beds amid the outbreak, South Korea imported an entire "Huoshenshan Hospital in slabs" from the Broad Group in China. The prefabricated stainless-steel slabs made up negative pressure isolation wards in South Korea. Equipped with fresh air systems and ozone technologies, the wards have the highest level of protection against cross infection. The project took only two days locally before the wards were put into use.






- Guangdong police prevent and recover billions from telecom fraud
- Chongqing rolls out late-night trains for Spring Festival travel
- Chinese healthcare innovations debut at World Health Expo Dubai 2026
- Senior CPC official stresses advancing peaceful relations across Taiwan Strait
- Shanghai hosts Spring Festival reception for intl media
- Former senior Chinese defense official charged with bribery















